Why Was Atenolol Taken Off The Market

Atenolol, a beta-blocker medication, was once a widely prescribed drug for managing hypertension (high blood pressure) and other cardiovascular conditions. However, its prominence has diminished significantly in recent years, with clinical guidelines increasingly recommending alternative treatments. While not entirely "taken off the market" in the strictest sense (it is still available as a generic medication), its usage is now far less common. This article explores the reasons behind this shift, focusing on evidence-based medicine and evolving clinical understanding.
Evolving Clinical Evidence and Treatment Guidelines
The decline in atenolol's popularity stems primarily from a growing body of evidence questioning its efficacy compared to other antihypertensive drugs. For many years, beta-blockers, including atenolol, were considered first-line treatments for hypertension. This recommendation was largely based on studies conducted in the 1970s and 1980s. However, more recent and comprehensive research has painted a different picture.
Specifically, studies have shown that atenolol may not be as effective as other classes of antihypertensive drugs, such as thiazide diuretics, ACE inhibitors (angiotensin-converting enzyme inhibitors), and ARBs (angiotensin II receptor blockers), in preventing cardiovascular events like stroke and heart attack. These newer trials often involved larger patient populations and longer follow-up periods, providing a more robust understanding of long-term outcomes.
Must Read
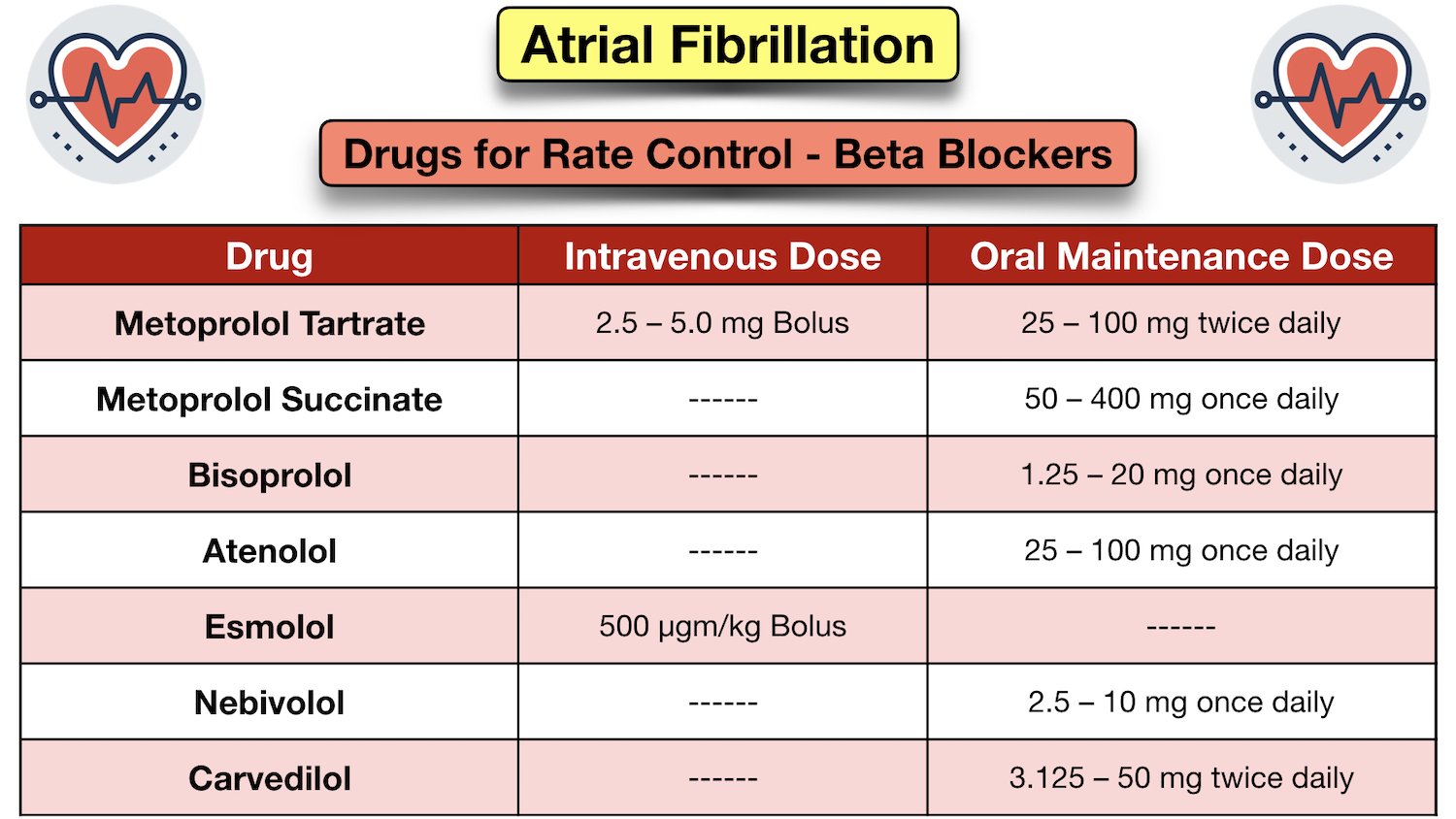
Clinical guidelines, such as those issued by the American Heart Association (AHA) and the American College of Cardiology (ACC), are regularly updated based on the latest scientific evidence. These guidelines now generally recommend thiazide diuretics, ACE inhibitors, ARBs, and calcium channel blockers as preferred initial treatments for hypertension in most patients. Atenolol and other beta-blockers are typically reserved for specific situations, such as when patients have co-existing conditions like angina (chest pain) or atrial fibrillation (an irregular heartbeat).
Key Studies and Meta-Analyses
Several key studies and meta-analyses have contributed to the re-evaluation of atenolol's role in hypertension management. One influential study was the ASCOT (Anglo-Scandinavian Cardiac Outcomes Trial), which compared a regimen of amlodipine (a calcium channel blocker) with or without perindopril (an ACE inhibitor) to a regimen of atenolol with or without bendroflumethiazide (a thiazide diuretic). The results showed that the amlodipine-based regimen was associated with a significantly lower risk of stroke and cardiovascular death compared to the atenolol-based regimen. This finding challenged the long-held belief that atenolol was a superior or equivalent choice for initial hypertension treatment.

Another important study was the LIFE (Losartan Intervention For Endpoint reduction in hypertension) study, which compared losartan (an ARB) to atenolol in patients with hypertension and left ventricular hypertrophy (enlargement of the heart's left ventricle). The study found that losartan was more effective than atenolol in reducing the risk of cardiovascular death, stroke, and myocardial infarction (heart attack). These findings further supported the use of ARBs over atenolol in certain patient populations.
Meta-analyses, which combine data from multiple studies, have also consistently demonstrated that atenolol may be less effective than other antihypertensive drugs in preventing cardiovascular events. These analyses provide a comprehensive overview of the available evidence and strengthen the conclusion that atenolol is not the optimal choice for many patients with hypertension.
Side Effects and Tolerability
In addition to concerns about its efficacy, atenolol is also associated with a higher incidence of certain side effects compared to some other antihypertensive drugs. Common side effects of atenolol include fatigue, dizziness, cold extremities, and erectile dysfunction. While these side effects are not life-threatening, they can significantly impact a patient's quality of life and adherence to treatment.

Furthermore, atenolol can have negative effects on glucose metabolism, potentially increasing the risk of developing type 2 diabetes, particularly in individuals who are already at risk. This is a significant concern, given the increasing prevalence of diabetes worldwide. Other beta-blockers, such as carvedilol and nebivolol, have been shown to have a more neutral or even beneficial effect on glucose metabolism, making them potentially preferable alternatives in patients with diabetes or pre-diabetes.
Compared to newer antihypertensive drugs, atenolol may also be less well-tolerated by some patients. For example, ACE inhibitors and ARBs are generally associated with fewer metabolic side effects and a lower risk of erectile dysfunction. This improved tolerability can lead to better patient adherence and ultimately, better blood pressure control.
Specific Clinical Scenarios Where Atenolol Remains Relevant
Despite the general trend away from atenolol as a first-line treatment for hypertension, there are still specific clinical scenarios where it may be a reasonable choice. These include:
- Angina: Atenolol can effectively reduce chest pain associated with angina by slowing down the heart rate and reducing the heart's workload.
- Atrial fibrillation: Atenolol can help control the heart rate in patients with atrial fibrillation, an irregular and often rapid heart rhythm.
- Migraine prophylaxis: In some cases, atenolol may be used to prevent migraines, although other beta-blockers like propranolol are often preferred.
- Hyperthyroidism: Atenolol can help manage the symptoms of hyperthyroidism, such as rapid heart rate and tremors.
- Essential tremor: Atenolol can reduce the severity of essential tremor, a neurological disorder that causes involuntary shaking.
- Compelling indications: If a patient has a specific compelling indication that favors the use of a beta-blocker and atenolol is well-tolerated and effective for that individual, it may still be an appropriate choice.
It is important to note that the decision to use atenolol should be made on a case-by-case basis, taking into account the patient's individual medical history, other medications, and potential side effects.
The Role of Cost and Availability
While clinical effectiveness and tolerability are the primary drivers behind the decline in atenolol's popularity, cost and availability also play a role. Atenolol is a generic medication and is therefore relatively inexpensive. This can be a significant advantage for patients who have limited financial resources or who lack adequate insurance coverage. In some healthcare systems, atenolol may be preferred over more expensive alternatives for economic reasons.
However, the cost advantage of atenolol is often outweighed by the potential benefits of other antihypertensive drugs, particularly in terms of long-term cardiovascular outcomes. While the initial cost of newer medications may be higher, the reduction in cardiovascular events can lead to significant cost savings in the long run, by reducing the need for hospitalizations and other medical interventions.

Furthermore, the availability of other generic antihypertensive drugs, such as thiazide diuretics, ACE inhibitors, and ARBs, has reduced the relative cost advantage of atenolol. These medications are now widely available and affordable, making them a more attractive option for many patients.
Conclusion
In summary, atenolol's decline in popularity as a first-line treatment for hypertension is primarily due to evolving clinical evidence demonstrating that it may be less effective than other antihypertensive drugs in preventing cardiovascular events like stroke and heart attack. Furthermore, atenolol is associated with a higher incidence of certain side effects compared to some alternatives. While atenolol still has a role in specific clinical scenarios, such as angina and atrial fibrillation, it is no longer considered the optimal choice for many patients with hypertension. The shift away from atenolol highlights the importance of evidence-based medicine and the ongoing need to re-evaluate treatment guidelines as new research emerges. By using the most effective and well-tolerated medications, healthcare professionals can help patients achieve better blood pressure control and reduce their risk of cardiovascular disease.
Why does this matter? Understanding why a once-common medication like atenolol has fallen out of favor is crucial for both healthcare providers and patients. It emphasizes the dynamic nature of medicine, where treatments are constantly being re-evaluated based on new evidence. This knowledge empowers patients to engage in informed discussions with their doctors about the best treatment options for their individual needs, promoting better health outcomes and ultimately saving lives by reducing the risk of debilitating cardiovascular events.