When Does Mounjaro Peak In Your System

Mounjaro (tirzepatide) represents a significant advancement in the treatment of type 2 diabetes. It functions as a dual glucose-dependent insulinotropic polypeptide (GIP) and glucagon-like peptide-1 (GLP-1) receptor agonist. Understanding its pharmacokinetic profile, particularly when it reaches its peak concentration in the system, is crucial for both healthcare professionals and patients to optimize its therapeutic benefits and manage potential side effects.
Pharmacokinetics of Tirzepatide
Pharmacokinetics describes how the body processes a drug, encompassing absorption, distribution, metabolism, and excretion (ADME). Tirzepatide is administered subcutaneously, typically once weekly. After injection, it is absorbed into the bloodstream. The rate and extent of absorption can influence the timing of peak concentration.
Absorption and Bioavailability
Subcutaneous administration allows for relatively slow and sustained absorption. The bioavailability of tirzepatide is approximately 80%, meaning that 80% of the administered dose reaches the systemic circulation. This is a key factor differentiating it from some older GLP-1 receptor agonists that may have lower bioavailability, necessitating more frequent injections.
Must Read
Time to Peak Concentration (Tmax)
The time to reach peak concentration (Tmax) for tirzepatide is generally observed between 24 to 72 hours post-injection. This relatively wide range can be attributed to individual variations in absorption rates, injection site, and subcutaneous tissue composition. Clinical trials have demonstrated that peak concentrations are typically attained within this timeframe across diverse patient populations.
Factors Influencing Peak Concentration Timing
Several factors can influence when Mounjaro reaches its peak concentration in the system. Understanding these variables is essential for tailoring treatment strategies and addressing individual patient needs.
Injection Site
The site of subcutaneous injection can impact absorption rates. Common injection sites include the abdomen, thigh, and upper arm. Studies have suggested that absorption from the abdomen may be slightly faster compared to the thigh. However, the differences are generally not clinically significant enough to warrant strict injection site rotation guidelines. Patients should be advised to consistently use the same injection site each week, as variations in absorption can affect glucose control.

Dosage
The dosage of tirzepatide directly influences the peak concentration. Higher doses will naturally lead to higher peak levels in the bloodstream. Mounjaro is typically initiated at a low dose (e.g., 2.5 mg) and gradually increased to the maintenance dose (e.g., 5 mg, 10 mg, or 15 mg) based on individual response and tolerability. The titration process aims to balance glycemic control with the risk of gastrointestinal side effects.
Individual Patient Characteristics
Individual patient characteristics such as body weight, age, renal function, and concomitant medications can also affect the pharmacokinetic profile of tirzepatide. For example, patients with impaired renal function may exhibit slower clearance of the drug, potentially leading to higher peak concentrations and a prolonged duration of action. However, studies have shown that mild to moderate renal impairment does not necessitate dose adjustments.
Concomitant Medications
While tirzepatide has a relatively low risk of drug-drug interactions, co-administration with certain medications, particularly those that affect gastric emptying, could theoretically influence absorption rates. For instance, medications that slow gastric emptying may delay the absorption of tirzepatide, leading to a later Tmax. However, the clinical significance of such interactions is generally considered to be minor.
Effects and Implications of Peak Mounjaro Concentration
The timing and magnitude of peak Mounjaro concentrations have several important clinical implications.
Glycemic Control
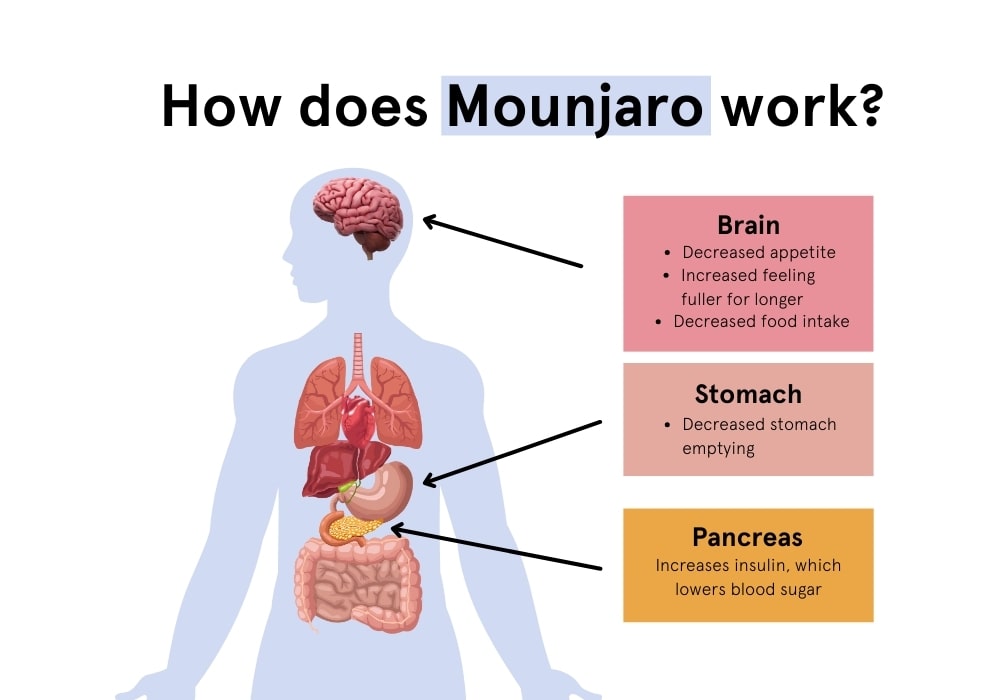
The peak concentration of tirzepatide is closely related to its glucose-lowering effects. After injection and reaching peak concentration, tirzepatide stimulates insulin secretion from pancreatic beta cells in a glucose-dependent manner. It also suppresses glucagon secretion, further contributing to improved glycemic control. The sustained release of tirzepatide over the week ensures consistent glucose management throughout the dosing interval.
Side Effects
Gastrointestinal side effects, such as nausea, vomiting, diarrhea, and constipation, are the most commonly reported adverse events associated with tirzepatide. These side effects are often more pronounced during the initial stages of treatment and when the dose is increased. The occurrence and severity of these side effects are often correlated with the peak concentration of the drug. Starting with a low dose and gradually titrating upwards can help mitigate these effects.
Weight Loss
Tirzepatide has also demonstrated significant weight loss benefits in clinical trials. The mechanisms underlying this effect are multifactorial and include reduced appetite, increased satiety, and delayed gastric emptying. While the exact relationship between peak concentration and weight loss is not fully elucidated, it is plausible that higher peak concentrations may contribute to greater appetite suppression.
Patient Education and Adherence
Understanding the pharmacokinetic profile of Mounjaro is critical for patient education and adherence. Patients should be informed about the expected timing of peak concentration, the potential side effects, and strategies for managing them. Encouraging patients to adhere to the prescribed dosing schedule and titration regimen is essential for optimizing therapeutic outcomes.
Comparison to Other GLP-1 Receptor Agonists
While Mounjaro is a dual GIP and GLP-1 receptor agonist, it is beneficial to compare it with GLP-1 receptor agonists. Semaglutide (Ozempic, Wegovy) is a GLP-1 receptor agonist also administered subcutaneously once weekly. Although both drugs have similar mechanisms of action in terms of GLP-1 agonism, tirzepatide's dual GIP agonism sets it apart. Studies suggest that tirzepatide may offer superior glycemic control and weight loss compared to semaglutide.
“In clinical trials, tirzepatide consistently demonstrated greater reductions in HbA1c and body weight compared to semaglutide, even at comparable doses. This is likely attributable to the synergistic effects of GIP and GLP-1 receptor agonism.” – Diabetes Care Journal
The pharmacokinetic profiles of these drugs also differ slightly. Semaglutide typically reaches peak concentration within 1 to 3 days after administration, similar to tirzepatide. However, the overall exposure to tirzepatide may be different because of its distinct ADME properties and the influence of GIP agonism.
Broader Significance
The development of Mounjaro represents a significant step forward in the management of type 2 diabetes. By targeting both GIP and GLP-1 receptors, it offers improved glycemic control and weight loss benefits compared to traditional GLP-1 receptor agonists. Understanding the pharmacokinetic profile of tirzepatide, including the timing of peak concentration and the factors that influence it, is essential for optimizing its therapeutic potential and minimizing adverse effects.
The insights gained from studying tirzepatide can also inform the development of future diabetes therapies. The concept of dual or multi-receptor agonists is gaining traction in the field, and further research in this area could lead to even more effective and personalized treatment strategies. As the prevalence of type 2 diabetes continues to rise globally, the need for innovative and effective therapies like Mounjaro is more pressing than ever. By understanding the intricacies of drug pharmacokinetics and individual patient characteristics, healthcare professionals can provide tailored treatment plans that improve outcomes and enhance the quality of life for individuals living with diabetes.