Genetic Testing For Long Qt Syndrome

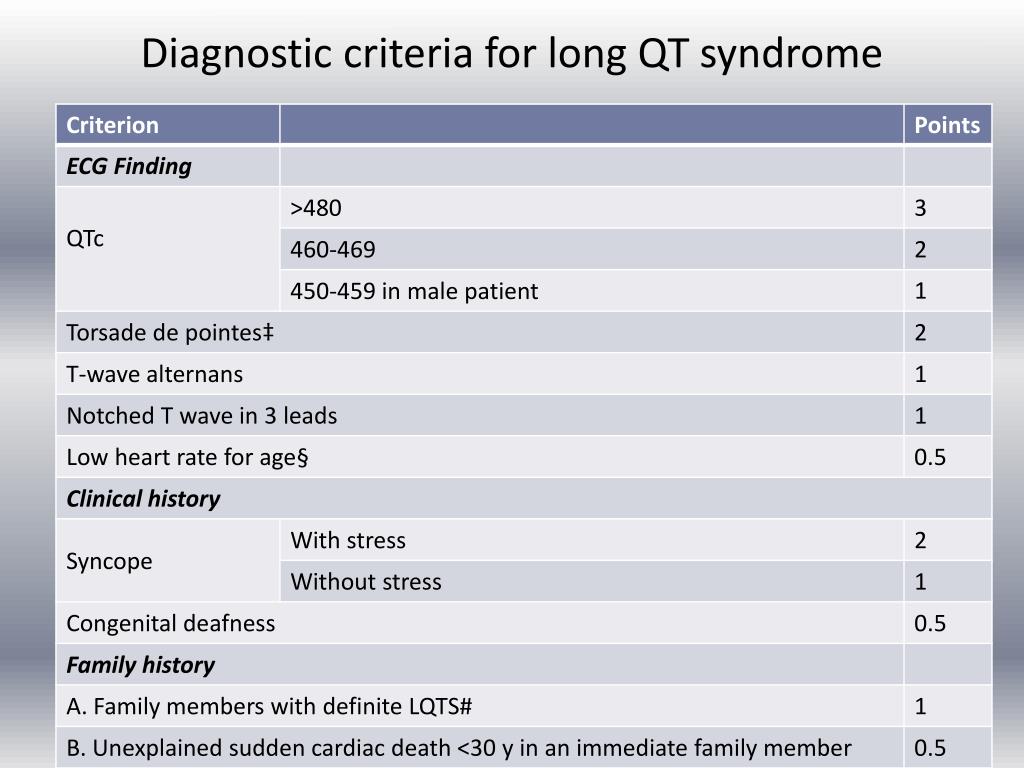
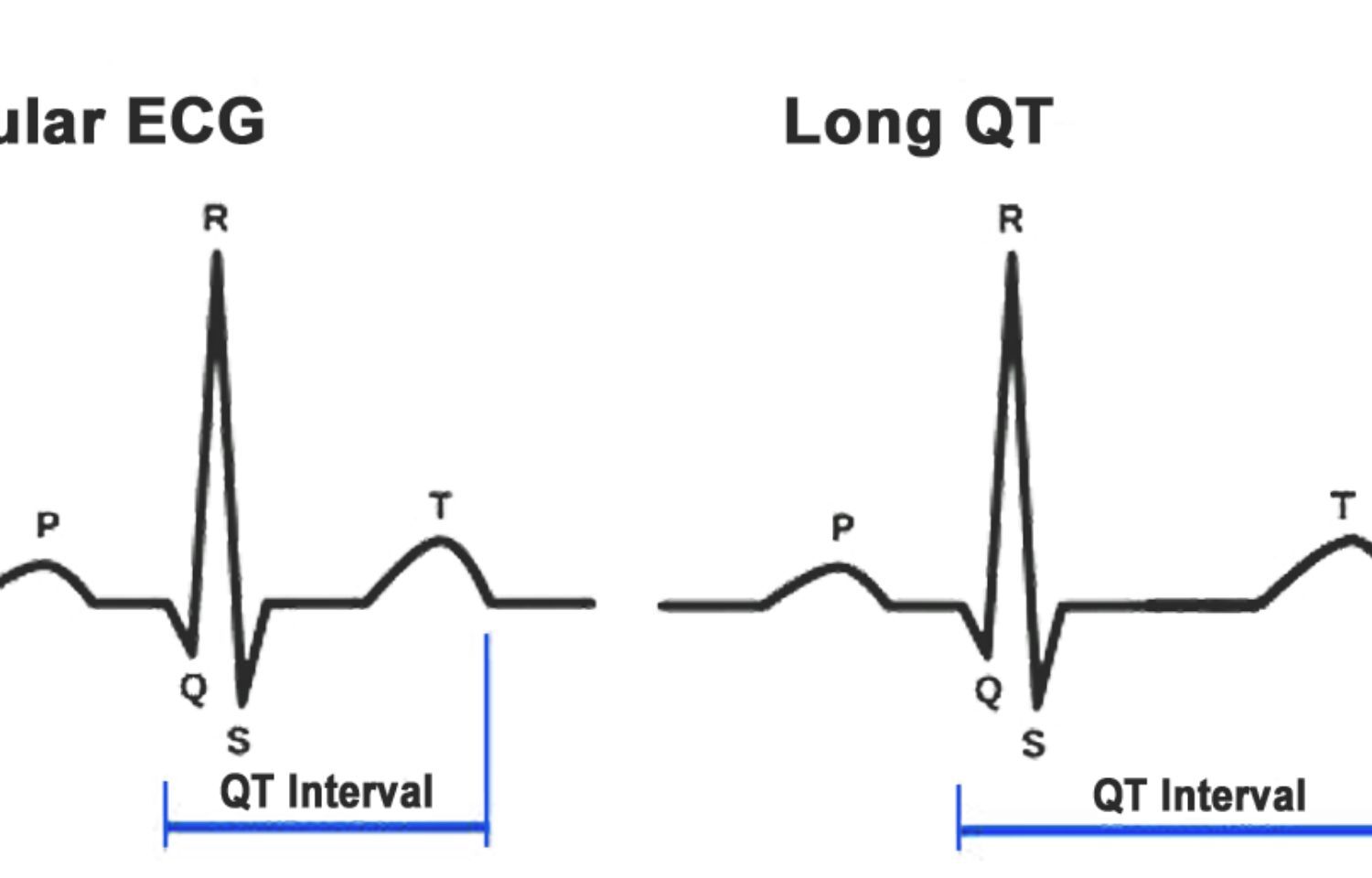
Long QT syndrome (LQTS) is a cardiac repolarization disorder characterized by a prolonged QT interval on the electrocardiogram (ECG), increasing the risk of potentially life-threatening ventricular arrhythmias, specifically torsades de pointes. While acquired forms of LQTS can arise from medication side effects or electrolyte imbalances, congenital LQTS is primarily caused by genetic mutations affecting ion channels in the heart.
Causes of Long QT Syndrome
The underlying cause of congenital LQTS lies in mutations affecting genes that encode cardiac ion channels or their associated proteins. These channels regulate the flow of ions (sodium, potassium, and calcium) into and out of heart muscle cells, which is crucial for the electrical activity that drives heartbeats. Mutations in these genes disrupt the normal repolarization process, leading to a prolonged QT interval.
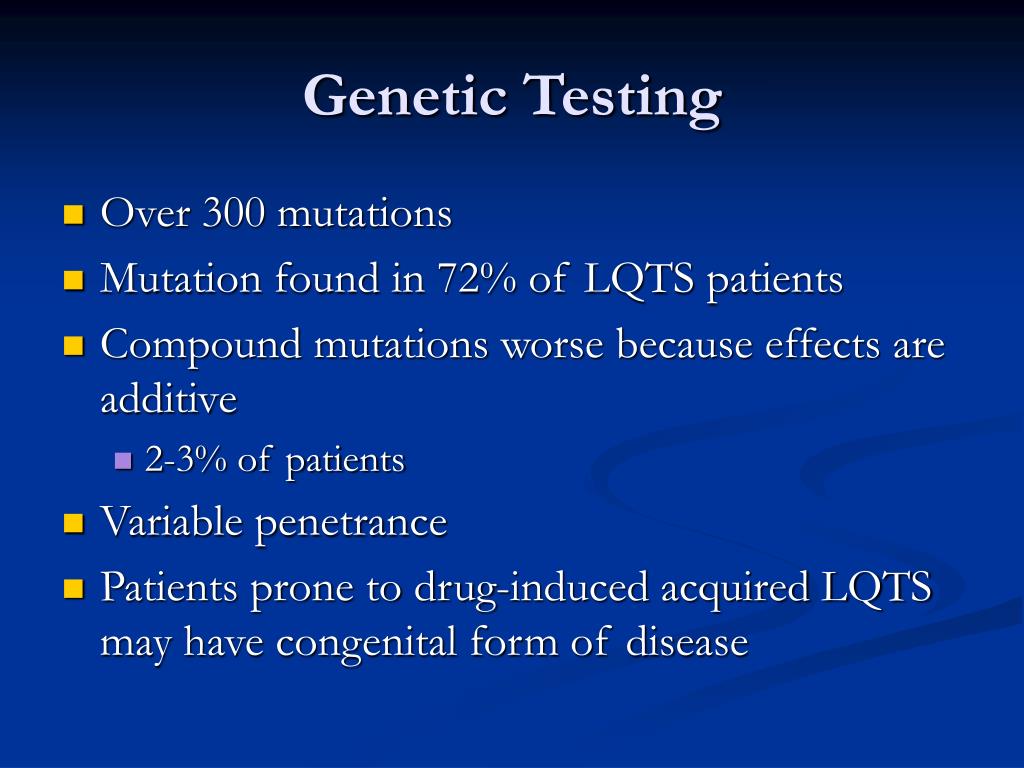
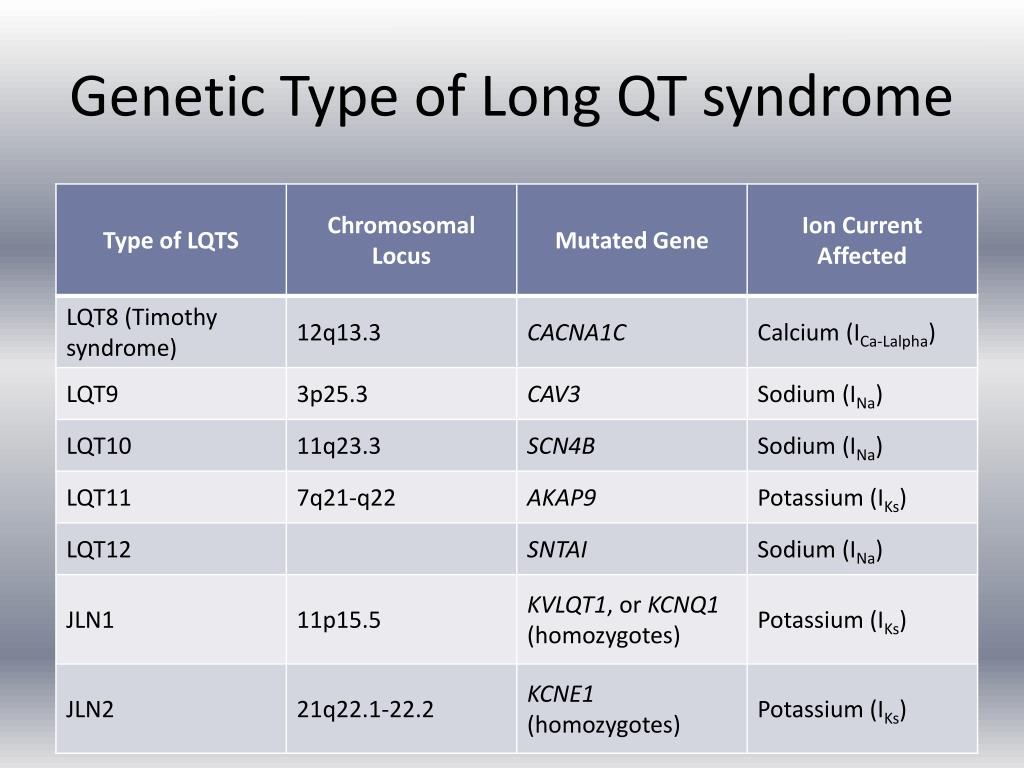
Currently, over 17 genes have been implicated in LQTS. The three most common genes account for approximately 90% of genetically identified cases. These are:
Must Read
- KCNQ1 (LQT1): This gene encodes the alpha subunit of the Kv7.1 potassium channel, responsible for the slow delayed rectifier potassium current (IKs). LQT1 is frequently triggered by exercise or emotional stress.
- KCNH2 (LQT2): This gene encodes the alpha subunit of the human ether-à-go-go-related gene (hERG) potassium channel, responsible for the rapid delayed rectifier potassium current (IKr). LQT2 is often triggered by auditory stimuli or during sleep.
- SCN5A (LQT3): This gene encodes the alpha subunit of the cardiac sodium channel (Nav1.5). LQT3 is often triggered during sleep or at rest and is associated with a higher risk of sudden cardiac death.
Other less common genes associated with LQTS include CALM1, CALM2, CALM3, ANK2, KCNE1, KCNE2, CACNA1C, CACNB2, SCN4B, AKAP9, SNTA1, HCN4, KCNJ5, and TRDN. Mutations in these genes typically result in more complex or atypical presentations of LQTS.
The inheritance pattern of LQTS is typically autosomal dominant, meaning that only one copy of the mutated gene is needed to cause the condition. However, autosomal recessive forms also exist, requiring two copies of the mutated gene. Furthermore, some individuals with LQTS may have a de novo mutation, meaning the mutation occurred spontaneously and was not inherited from their parents.
Effects of Long QT Syndrome
The primary effect of LQTS is an increased susceptibility to ventricular arrhythmias, particularly torsades de pointes. Torsades de pointes is a polymorphic ventricular tachycardia characterized by a twisting of the QRS complexes around the isoelectric baseline on the ECG. This arrhythmia can lead to palpitations, dizziness, fainting (syncope), and, in severe cases, sudden cardiac death.
The risk of experiencing a cardiac event varies significantly among individuals with LQTS. Factors influencing risk include the specific gene mutation, the degree of QT prolongation, age, sex (females generally have a higher risk), and the presence of other medical conditions. For example, individuals with LQT3 are often considered to be at higher risk than those with LQT1 or LQT2.
Symptoms of LQTS can be highly variable. Some individuals may be asymptomatic and only diagnosed after a routine ECG or after genetic testing prompted by a family history of sudden death or LQTS. Others may experience recurrent episodes of syncope, often triggered by specific stimuli depending on the genetic subtype. In some cases, the first manifestation of LQTS can be sudden cardiac death, highlighting the importance of early diagnosis and management.
The impact of LQTS extends beyond the immediate physical risks. Individuals with LQTS may experience anxiety and fear related to the possibility of a cardiac event. Lifestyle modifications, such as avoiding certain medications and strenuous activities, can also affect their quality of life. Furthermore, the diagnosis of LQTS in a family can have significant psychological and social implications for all members, prompting cascade screening and potentially altering life choices.
Implications of Genetic Testing
Genetic testing plays a crucial role in the diagnosis and management of LQTS. It offers several important benefits:
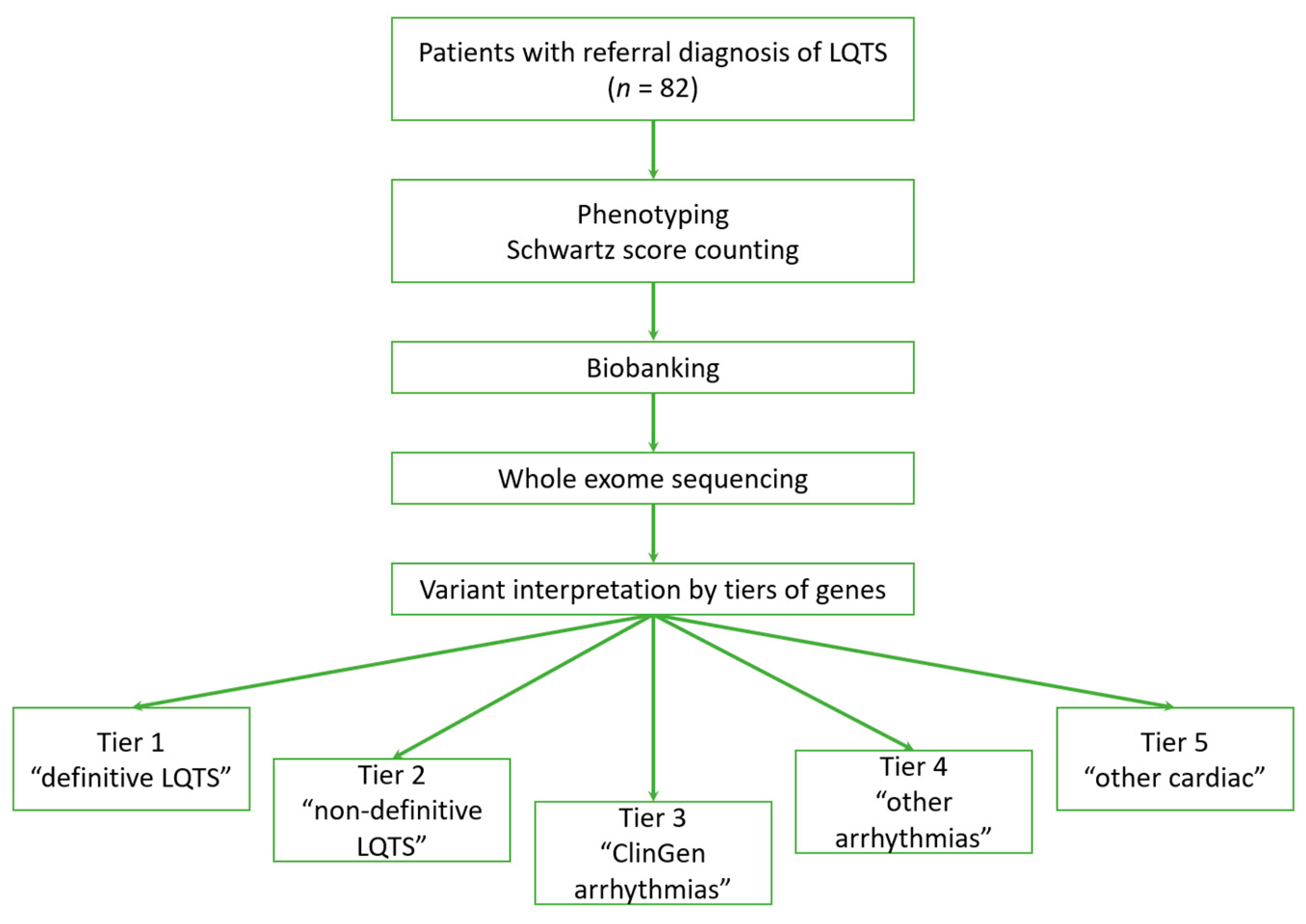
- Confirmation of Diagnosis: Genetic testing can confirm the diagnosis of LQTS in individuals with a prolonged QT interval on ECG, especially when clinical findings are ambiguous.
- Risk Stratification: Identifying the specific gene mutation can help to assess the risk of future cardiac events. Certain mutations are associated with a higher risk of arrhythmias and sudden death, allowing for more targeted management strategies.
- Family Screening: Genetic testing allows for cascade screening of family members. Identifying individuals with the same mutation, even if they are asymptomatic, allows for early intervention and preventative measures, such as lifestyle modifications, medication, or implantable cardioverter-defibrillators (ICDs).
- Personalized Management: Knowledge of the specific genetic subtype can guide treatment decisions. For example, beta-blockers are generally effective for LQT1 and LQT2, but less so for LQT3, where sodium channel blockers may be more appropriate.
- Reproductive Counseling: Genetic testing provides information for reproductive counseling, allowing families to understand the risk of transmitting the condition to their children and explore options such as preimplantation genetic diagnosis (PGD).
However, genetic testing for LQTS also has limitations:

- Incomplete Gene Coverage: Current genetic testing panels may not include all known genes associated with LQTS. Therefore, a negative genetic test does not completely rule out the diagnosis, especially if clinical suspicion is high.
- Variants of Uncertain Significance (VUS): Genetic testing may identify variants of uncertain significance (VUS), where the effect of the mutation on ion channel function is unknown. Interpreting VUS can be challenging and may require further functional studies.
- Phenotypic Variability: Even within the same family with the same mutation, there can be significant variability in the severity of LQTS. This highlights the role of other genetic and environmental factors in modulating the phenotype.
- Psychological Impact: A positive genetic test can cause anxiety and distress, particularly if the individual is asymptomatic. Careful counseling and support are essential.
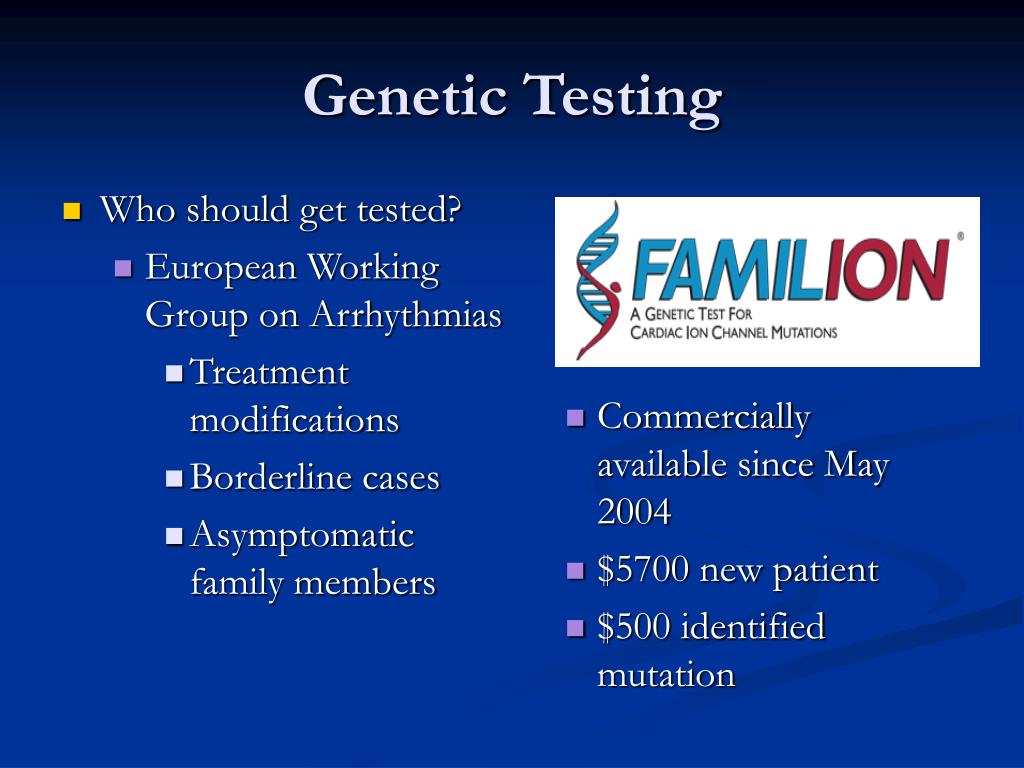
The cost of genetic testing can also be a barrier to access, although it has decreased significantly in recent years. Furthermore, ethical considerations, such as privacy and potential discrimination based on genetic information, need to be addressed.
According to a 2017 study published in the journal Circulation, genetic testing identified a causative mutation in approximately 75% of clinically diagnosed LQTS patients. This demonstrates the significant, but not complete, diagnostic yield of genetic testing in this population. As technology advances and more genes are discovered, the diagnostic yield is expected to increase.
Broader Significance
Genetic testing for LQTS exemplifies the increasing role of personalized medicine in cardiology. By understanding the genetic basis of this condition, clinicians can provide more accurate diagnoses, better risk stratification, and tailored treatment strategies. The ability to identify asymptomatic individuals at risk allows for proactive interventions that can prevent life-threatening arrhythmias and improve outcomes. The integration of genetic information into clinical decision-making is transforming the management of LQTS and other inherited cardiac conditions.

Furthermore, the study of LQTS has contributed significantly to our understanding of cardiac electrophysiology and ion channel function. Mutations in LQTS genes have provided valuable insights into the molecular mechanisms underlying cardiac arrhythmias. This knowledge has implications for the development of new therapies for LQTS and other cardiac disorders.
The broader implications of genetic testing for LQTS extend beyond cardiology. It highlights the potential of genetic testing to improve the diagnosis and management of a wide range of inherited diseases. As genetic technologies become more accessible and affordable, they are likely to play an increasingly important role in healthcare. However, it is crucial to address the ethical, legal, and social implications of genetic testing to ensure that it is used responsibly and equitably.
In conclusion, genetic testing for Long QT Syndrome is a powerful tool that offers significant benefits for diagnosis, risk stratification, family screening, and personalized management. While limitations exist, the continued advancement of genetic technologies and our understanding of the genetic basis of cardiac arrhythmias will further enhance the impact of genetic testing on the lives of individuals and families affected by LQTS.